Probleemstelling:
Physical exercise is considered protective in terms of major adverse cardiovascular events (myocardial infarction stroke). Less known, however, - and paradoxical - is that the extent and prevalence of coronary atherosclerosis is higher in athletes. To investigathe this intruiging phenomenon in more depth, the research team of Dr. Guido Claessen, cardiologist at University of Hasselt, designed the Master@Heart study which includes 191 lifelong master endurance athletes, 191 late-onset athletes (endurance sports initiation after 30 years of age), and 176 healthy non-athletes, all male with a low cardiovascular risk profile. The primary endpoint was the prevalence of coronary plaques (calcified, mixed, and non-calcified) on computed tomography coronary angiography.
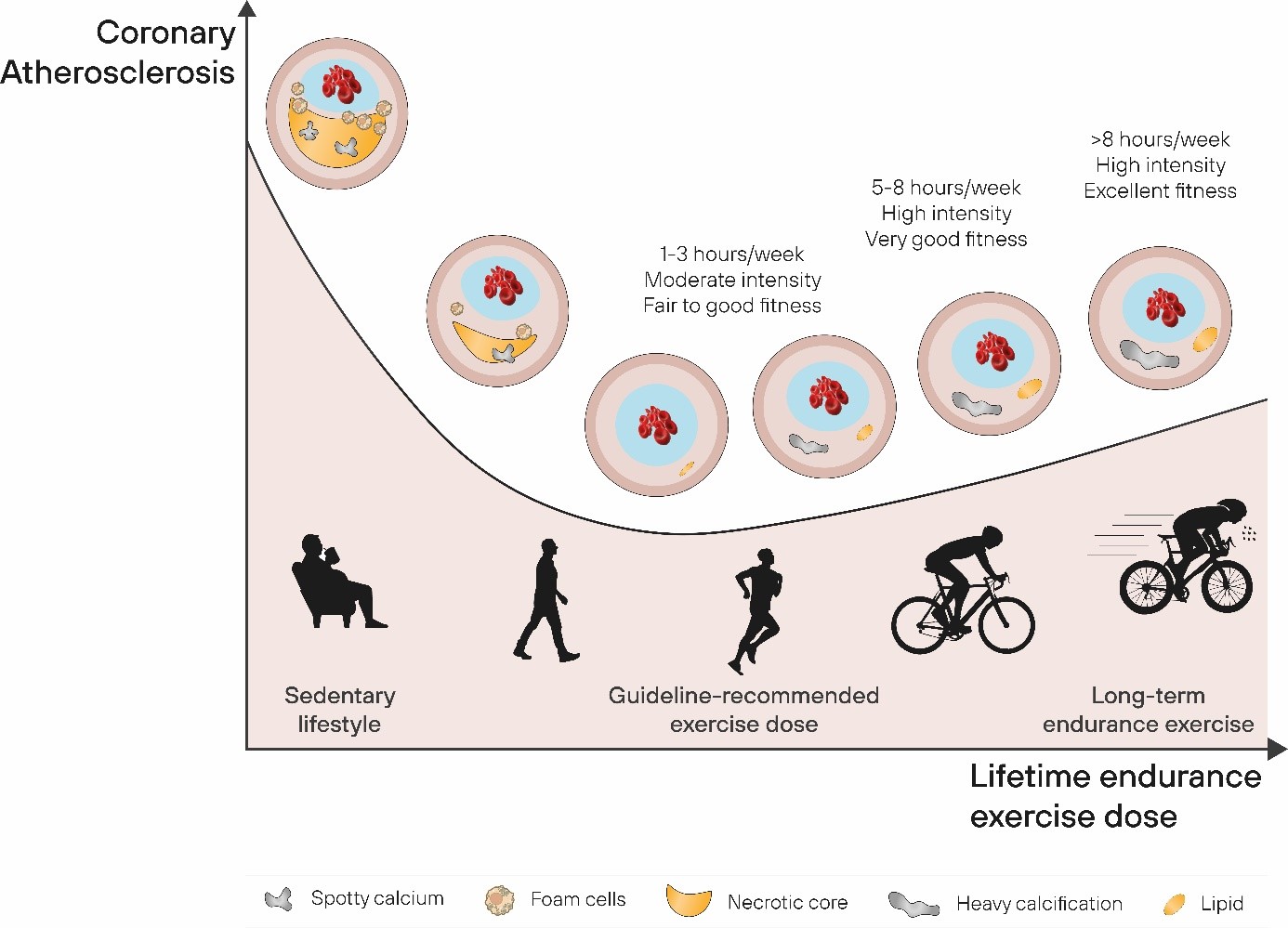
Considering that a higher exercise aerobic power, so-called VO2max, is associated with a lower lipid volume, higher fibrous volume, and thicker fibrous cap in coronary plaques, we speculate that the dose-response relationship between endurance exercise and coronary atherosclerosis might be reverse J-shaped rather than a descending logarithmic function (See figure, left panel). A sedentary and unhealthy lifestyle carries the highest risk of ischemic heart disease with a significant burden of high-risk plaques. Conversely, a lower prevalence of cardiac risk factors with low physical activity levels is associated with reduced coronary atherosclerosis but unfavourable plaque characteristics. Our Master@Heart data demonstrate that a healthy lifestyle and above-average cardiorespiratory training and fitness prevents coronary atherosclerosis with a more favourable pattern of more calcified and less mixed or soft plaques. Additional increments of endurance sports training load and associated increases in fitness do not affect the distribution of plaque types. However, lifetime intensive endurance training increases the overall coronary atherosclerotic burden with more plaques, including soft and mixed plaques, plaques in proximal segments and those with a significant degree of stenosis.
Until present, the mechanisms underpinning the increased plaque burden remain unknown. A better understanding of the pathophysiological process would be highly desirable though given the acute coronary events are the leading cause of sudden cardiac death in physically active individuals beyond the age of 35 and the observed increase of the average age of endurance race participants. A substantial subset of calcified plaques in human athletes are situated in the proximal segments of the coronary artery tree, and this anatomical predisposition may indicate that biomechanical factors play a role in the disease process, such as stresses within the wall, or the shear stress that is exerted on the eondothelial cells.